All published articles of this journal are available on ScienceDirect.

Tinnitus: A Tingling Mystery to be Decrypted
Authors Info & Affiliations
Abstract
Tinnitus is a hearing disorder that causes ringing, buzzing or hissing sensation to the patient’s auditory senses. It has become a very common complaint over the years affecting around 7-8% of the human population all over the world. The disorder causes the patients to feel irritable, annoyed, depressed, and distressed. As a result, it obstructs their sense of relaxation, enjoyment, and even their sleep - thus forcing them to avoid any social gatherings. There has been a substantial amount of work that has been carried out pertinent to this disorder. This paper reviews existing research and work done regarding Tinnitus effects, causes, and diagnosis. The numerous ways in which Tinnitus could affect an individual have been depicted. From the plethora of probable causes of this disorder, the most conceivable ones are highlighted. Moreover, this paper documents and reviews the attempts at treating Tinnitus, relevant engineering breakthroughs, and the various ways in which Tinnitus noise is suppressed – such as Tinnitus Retraining Therapy, Neuromodulation, and Signal processing approach. The manuscripts highlight the pros and cons of these methods. Over 45 research articles and other reliable internet medical sources were reviewed and these pieces of work were contrasted. These findings should help in understanding both – the disorder, as well as the situation of the patients suffering from it. Through this manuscript, an attempt was made to spread awareness about the mysterious disorder.
1. INTRODUCTION
Tinnitus is a perception of noise in the head and/or in the ear, having no external source.
It is derived from the Latin word ‘tinnire’ which means to ring [1]. It is due to malfunctioning in the cochlea or malfunctioning of the nerves running from the ear to the head [2, 3]. The perceived noises can be categorized as ringing, buzzing, hissing, whistling, or some other noise. It may also be a combination of the aforementioned sounds [1]. Moreover, it may either be continuous or occur at irregular intervals. In quiet places, the amplitude of Tinnitus can be higher as compared to other places. It can either be felt in a single ear or both the ears. Sometimes, it may also be felt inside the head. These noises can be low, medium, or high pitched. It has been reported that some patients perceive the sound as the sound of heartbeats, water droplets, etc [4]. Almost everyone has experienced a short faint ringing noise in the ears at some point in time or others may notice it after hearing loud music or even when one spins around. All such noises are categorized as Tinnitus. However, it goes unnoticed in most of the people because it is neither continuous nor severe and also, at times, it is suppressed due to the loud environmental noises.
Tinnitus cannot be categorized as a disease or illness; it is a symptom that is mostly generated in the auditory system of the body. It is a very common problem and is generally reported in almost all age groups, even in young children. According to the National Centre for Health Statistics report [5], around 32% of the USA population faces Tinnitus and among them 6% deal with a severe degree of it. According to a survey by the British Tinnitus Association, about 30% of the people face Tinnitus at some point in their life and almost 10% of them remain consistent with Tinnitus [6]. The main reason and pathological background for Tinnitus are still not understood completely.
Demographically, Tinnitus is found to affect various age groups at different degrees [7]. The following chart shows the statistics (Fig. 1).
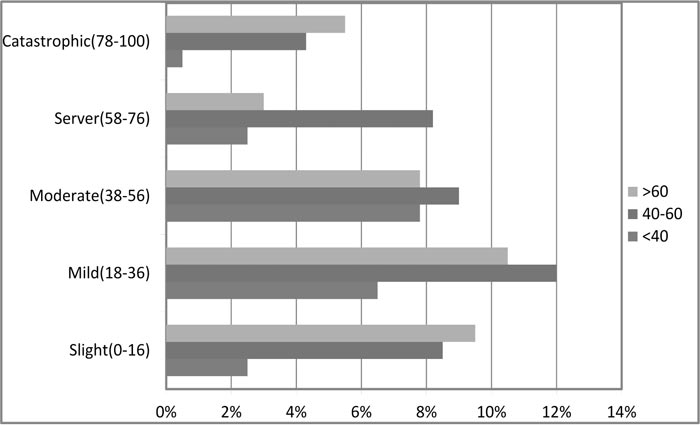
The survey [7] concludes that the presence of Tinnitus has been reported to progressively increase with age, affecting 5% of individuals, at 20–30 years of age and 12% of individuals above 60 years of age. The prevalence of Tinnitus increases to 70–85% in the hearing-impaired population [6]; 40 to 60-year-old individuals were most commonly affected, followed by individuals above 60 years of age, followed by individuals below 40 years of age. In most cases, Tinnitus is a result of some exposure to excessively loud and high pitched noises or may even be caused due to an accident. But for aged people, it is generally accompanied by hearing loss. One group of people who are in maximum affinity to attain Tinnitus are those who serve the army on the battlefields because they are subjected to loud noises for most of the time.
Broadly, Tinnitus is divided into two categories: (1) Subjective Tinnitus – in which only the person with Tinnitus can hear the sounds and (2) Objective Tinnitus – in which the person with Tinnitus and people around him/her can also hear the sounds. Subjective Tinnitus is very common but is difficult to evaluate; it is measured, quantified, and described only based on the patient’s response [8]. It is caused within the cochlea or in the subsequent stages of the auditory cortex. On the other hand, objective Tinnitus can be heard through a stethoscope placed overhead and neck structures near the patient’s ear. It is either caused due to vascular phenomenon or muscle changes, for example, the spasm of the muscle of the middle ear or palate. It usually ranges within the frequency range of 6-8 kHz without external sounds and for this reason, reliable measures of Tinnitus are very difficult and require sophisticated techniques. Despite patients' occasional descriptions of immensely loud sounds, it is seen that Tinnitus occurs at intensities of around 5-10dB above the normal hearing threshold.
Tinnitus a very common aural neurological symptom [4]. It is different from hallucinations in the sense that it is supposedly a sound that comes into being from the outside without any stimulation.
At present, there is no permanent cure for Tinnitus which can completely eradicate the cause of it. However, there are certain technologies like hearing aids, sound therapies, Tinnitus maskers that are used but with very little success. There are also a few drugs that claim to reduce the effect of Tinnitus up to a certain extent. A person suffering from both Tinnitus as well as hearing problems can use hearing aids available in the market, which not only help in hearing but also provide white noise whenever there is an episode of Tinnitus. This white noise tends to calm the person down.
In some technologies, people use a headset that they wear on a bald head that sends electrical impulses to suppress the effect of Tinnitus. According to Cochrane Library, a certain type of drug called Selective Serotonin Reuptake Inhibitor, which is an anti-depressant, reduces the severe effects of Tinnitus like anxiety and depression, but with prolonged use, it shows side effects like sedation, sexual dysfunction, and dry mouth [8, 9].
Nowadays meditation, yoga, and some relaxation therapy are being implemented to help the patient to cope up with the disturbance caused by Tinnitus. On the other hand, most Tinnitus patients are taught to live with it and get accustomed to it so that it does not affect their daily activities. This method is called Tinnitus Retraining Therapy (TRT) [10].
It must, however, be noted that none of the above-mentioned solutions provide a permanent cure to Tinnitus. The mentioned methods are further discussed in detail over the latter sections.
The paper is organized into three primary sections. The first section enumerates the various possible causes of Tinnitus. The next section highlights the impacts and adverse effects caused due to Tinnitus on the patient. The section following that elaborates on the engineering technologies deployed for various attempts at curing Tinnitus and literature on work pertinent to Tinnitus treatment. Lastly, a section on discussions is presented to summarize the literature and findings.
2. PATHOPHYSIOLOGY AND CAUSES OF TINNITUS
The pathophysiology of Tinnitus is still not completely understood and could be considered as one of the most controversial issues in medical science [11]. The American Tinnitus association [10] enumerates several possible causes of Tinnitus, including sensor neural hearing loss, which is commonly accompanied by Tinnitus. This includes age-related hearing loss and noise-induced hearing loss. The exact biological process by which hearing loss is associated with Tinnitus is still being investigated by researchers [12, 13]. However, what we do know is that the loss of certain sound frequencies leads to certain changes in how the brain processes sound. It has also been noted that:
- Blockages in the ear canal can give rise to Tinnitus. These blockages arise from excessive ear wax, head congestion, loose hair from the ear canal, dirt, and/or foreign objects. These lead to pressure build-up in the inner ear affecting the operation of the eardrum. The removal of these blockages may relieve the patient of Tinnitus symptoms unless in certain cases where permanent damage has been caused by the blockage, leading to chronic Tinnitus.
- A severe injury in the head-neck region has also been shown to result in the perception of Tinnitus due to issues caused by nerve, muscle, and flow of blood. The Tinnitus caused as a result of this has often been reported to be of higher volume and greater variability in frequency, sound, as well as the location of the noise. Tinnitus pertinent to this type is sometimes referred to as somatic Tinnitus [12]. Somatic Tinnitus includes the perception caused due to Temporomandibular Joint Disorder (TMJ) in which damage in the muscles, cartilage, or ligaments in the region connecting the lower jaw to the skull causes a perception of this noise. This region shares certain nerve connections with structures in the middle ear.
- Nasal congestion may also create abnormal pressure in the middle ear, giving rise to Tinnitus symptoms. This pressure can also be caused by other reasons for extreme/rapid changes in air pressure (or water pressure). Such activities include diving, flying, snorkeling, etc.
- Traumatic brain injury and consumption of ototoxic (including antibiotics such as gentamicin, streptomycin, tobramycin, loop diuretics such as furosemide, and platinum-based chemotherapy agents, such as cisplatin, carboplatin, and vincristine) drugs have also been reported to give rise to Tinnitus.
Listed above are the commonly reported and researched causes. There are a few other speculations and studies as well, however, a direct correlation and pathophysiology are yet to be constructed. A list of possible causes of Tinnitus is shown in Table 1.
Josef Rauschecker et al. [14] proposed a testable model for Tinnitus that is backed by results from human brain imaging and focuses on brain areas in the cortex, thalamus, and ventral striatum. According to the proposed model, Tinnitus most likely results from the following factors:
(1) A lesion to the auditory periphery, e.g., loss of hair cells in the inner ear resulting from acoustic trauma or aging – in most, if not all cases
(2) Loss of input in the lesioned frequency range leads to an over-representation of lesion-edge frequencies, which causes hyperactivity and possible burst-firing in central auditory pathways, constituting the initial Tinnitussignal.
(3) Under normal circumstances, the Tinnitus signal is canceled out at the level of the thalamus by an inhibitory feedback loop, originating in paralimbic structures: activity from these structures reaches the Thalamus Reticular Nucleus (TRN), which, in turn, inhibits the Medial Geniculate Nucleus (MGN). If, however, paralimbic regions are compromised, inhibition of the Tinnitus signal at the thalamic gate is lost, and the signal is relayed to the auditory cortex, where it leads to permanent reorganization and chronic Tinnitus.
The research opened pathways for drug treatment of Tinnitus by identifying the transmitter systems involved in the brain’s intrinsic NAc/vmPFC-TRN noise cancellation system.
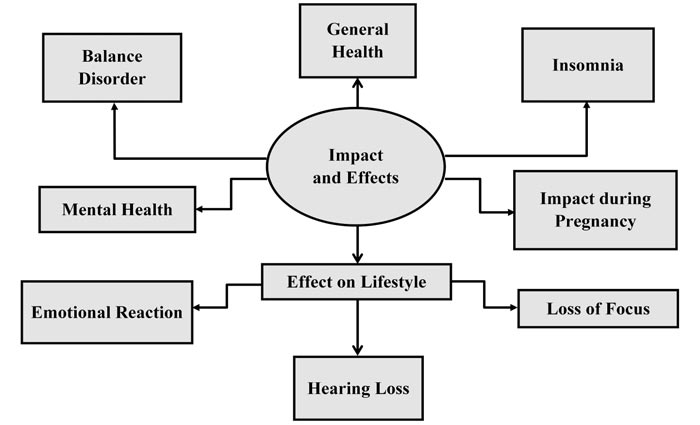
3. IMPACT AND EFFECTS OF TINNITUS:
This section discusses the plethora of effects that the disorder has on human activity, health, and lifestyle. Fig. (1-3) summarizes the various impacts and effects of Tinnitus.
| S. No. | Possible Cause |
|---|---|
| 1. | Age-related hearing loss |
| 2. | Noise-Induced hearing loss |
| 3. | Ear blockages and head congestions |
| 4. | A severe injury in the head-neck region |
| 5. | Temporomandibular Joint Disorder (TMJ) |
| 6. | Nasal Congestion and other causes for abnormal pressure build-up in the middle ear |
| 7. | Traumatic brain injury |
| 8. | Consumption of ototoxic drugs |
3.1. General Health
Continuous sounds of Tinnitus tend to irritate the person resulting in a lack of concentration towards their work. As a result, they may not be able to complete their work on time, which will increase the stress and anxiety level [15]. At the same time, it results in loss of sleep and a tendency to skip meals, which gives rise to fatigue and complete loss of efficiency. All these factors lead to the deterioration of their health.
3.1.1. Mind
Tinnitus is related to a part of the brain called the precuneus. The precuneus is connected to two other networks in the brain, known as the “dorsal attention network” and the “default mode network”. The default mode network handles background activities during rest or relaxation; on the other hand, the dorsal attention network recognizes stimulants like noises and touch. When something captures someone’s attention, their dorsal attention network kicks in. Otherwise, their brain adjusts to let the default mode network take over. This system allows people to relax their minds and reduce mental fatigue. However, when a person is suffering from Tinnitus, their brain focuses on the ringing. This prevents them from lapsing into default mode, which is unhealthy for the mind [16].
Tinnitus can increase a person’s risk of developing mental illnesses, including depression, anxiety, and can also trigger episodes of extreme anger and suicidal thoughts. The consistency of Tinnitus and the perceived lack of control can provoke fear, which increases the problem leading to an everlasting cycle of distress. According to a study published by JAMA, 11.4% of adults who suffer from Tinnitus have moderate to severe cases of depression [17]. Many people suffering from Tinnitus find it difficult to maintain concentration for prolonged periods as a lot of energy is drained in the annoying sound within the ears. As a result, he/she will not be able to complete their work on time and will lead to frustration, and, at times, this might go to the extent of suicide.
3.1.2. Insomnia
Mild sleep disturbances are very common, but to be classified as insomnia, the delay in falling asleep needs to be ample, occurring at least three or four times a week and persisting for at least six months. Insomnia and Tinnitus can feed off from each other in a vicious cycle. People who lose their sleep might worry about Tinnitus more and worrying about it can, in turn, cause a lack of sleep and restlessness [18].
Many people with Tinnitus do fall asleep, sleep well, and see sleep as a refreshing escape from Tinnitus. Those who sleep well at night generally do not seem to have different Tinnitus from those who face troubled sleeping. But those who have disturbed sleep worry more at night time than people with Tinnitus who sleep well. The worries that people have about the quantity of sleep or about the effects of not sleeping or about Tinnitus in general, have more of an impact on sleep problems than the sound of Tinnitus.
3.1.3. Effect During Pregnancy
Tinnitus effect during pregnancy is more common than in the general population. It is one of the most common ear complaints reported during pregnancy affecting over 1 in 3 women, as compared to just 1 in 10 women of the same age group who are not pregnant. Furthermore, 2 out of 3 women who have had Tinnitus before their pregnancy reported an increase in the amount of pain or difficulties during pregnancy. For those who suffer from Tinnitus for the first time during their pregnancy, it generally resolves or reduces after delivery [19].
The nerve cell present in the cochlea converts vibrations caused by sound waves into electrical impulses that travel via the auditory nerve into the brain. Physical changes that occur during pregnancy that interfere with this sensitive process can account for the new or increased perception of Tinnitus. For example, changes that occur during the pregnancy include a normal increase in circulating blood volume and also an increase in the pressure transmitted directly to the fluid inside the cochlea [20]. This fluid regulates electrical impulses from the inner ear to the brain and therefore, change in pressure in the cochlea may lead to alterations in these electrical impulses and the perception of Tinnitus.
Another mechanism that triggers Tinnitus is the natural retention of salt and water, which occurs during pregnancy. This can cause localized swelling and, thus, lead to the alteration of electrical impulses between the ear and the brain and affecting Tinnitus. Pregnancy is a time for both physical and emotional demand for every woman and the first time occurrence of Tinnitus or the increase in its’ level after pregnancy can be alarming for both the mother and the child. During Tinnitus, the mother may go through pain and stress which will affect her as well her child’s health. It is also likely to have high blood pressure, and Tinnitus may be an early sign of gestational hypertension, which leads to less supply of blood and oxygen to the baby and can lead to low birth weight of the baby. If it is severe, it leads to preeclampsia, which adversely affects the mother and the baby [20].
3.1.4. Balance Disorder
The inner ear is an intricate part of the human body that is crucial in maintaining the equilibrium by being sensitive to motion. The nerve endings in the vestibular region transfer the nerve impulses to the brain and help it to assess the body’s position and balance accordingly.
The control of balance in humans is quite complex and involves the coordination of several sensory systems. These are the musculoskeletal system, vision, and the balance organs in the internal ears. These systems are linked to a center at the base of the brain - the vestibular nucleus. This, in turn, sends information to, and also receives input from a nearby organ the cerebellum. The coordination of posture and balance is carried out by the cerebellum [21].
A disorder that occurs when there is a malfunction in the balance organs is known as Meniere’s disease. Hence attacks of dizziness are often accompanied by nausea, vomiting, hearing loss, and Tinnitus. These attacks may last as long as 24 hours, and are sometimes so severe that people may need admission to the hospital. After this, there is a gradual recovery of balance function and this might take several days. However, further attacks may occur during this period, and this may prolong the recovery process [22]. Fluid builds up inside a part of inner ear called the labyrinth, which holds structures that help with hearing and balance. The extra fluid interferes with the signals that brain receives, causing vertigo and hearing problems.
Thus, Tinnitus is one of the main reasons for balance disorders. But the disorder is significant only when the level of Tinnitus disturbance is greater than a threshold, which differs from person to person.
3.2. Effect on Lifestyle
The human impact of Tinnitus is beyond just the patient. It may affect the patient’s family, friends, and even co-workers in the process of supporting the patient. Those who intend to help often surpass their limit of patience, irritability, and confusion as they struggle to understand and help the Tinnitus patient, thus, the gap increases.
Some of the ways Tinnitus can affect the lifestyle are mentioned below:
- Hearing Loss: Many people who have Tinnitus also experience hearing loss. If the patient struggles to hear, it can make it difficult to follow conversations, get involved in meetings, and less inclined to socialize. If one cannot hear very well and is also prone to bouts of Tinnitus, it can have a significant impact on the way they live their life. They may become more isolated, and even the simplest daily tasks may become more daunting [24]. On experiencing more frequent symptoms of Tinnitus, or being worried about hearing loss, one must not hesitate to contact a hearing care provider. It is always beneficial to try and address problems as quickly as possible.
- Loss of Focus and Concentration: Tinnitus can make it hard to concentrate. Tackling complex tasks can become a huge issue. Tinnitus can affect one’s performance at work. On experiencing insomnia as a result of Tinnitus, concentration is further hampered due to a lack of sleep.
- Emotional Reaction: At first, the sound is distracting. If the sound persists, it can become annoying. This type of cycle tends to happen with Tinnitus. Emotional reactions can include frustration, worry, and anger. Some people report anxiety or depression because of Tinnitus. As mentioned above, the effects of Tinnitus usually include emotional reactions. For this reason, Tinnitus management should focus on managing these reactions [25-27].
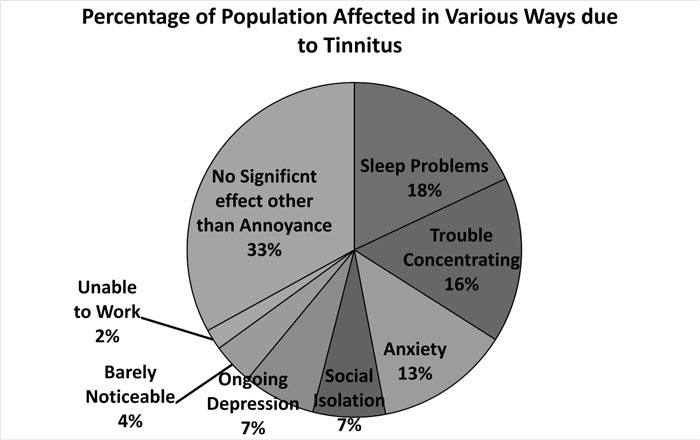
The statistical information on various effects of Tinnitus [23] on human life is shown in Fig. (4).
4. ENGINEERING BREAKTHROUGHS AND TREATMENT PROCEDURES
Engineering is nothing but the application of scientific and mathematical techniques to solve problems in various use-cases. It finds extensive applications in various branches of medicine. Cases of Tinnitus have also, to some extent, been alleviated due to engineering breakthroughs. This section gives a brief account of engineering technologies and discoveries that have been applied to treat and suppress Tinnitus.
As mentioned earlier, there has been no permanent cure for Tinnitus. Rather, there are various methods for suppressing Tinnitus noise, of varied effectiveness. Tinnitus often accompanies other clinical hearing disorders. Because of this, some therapies are based on operative techniques and the cochlea implant hearing aids are also used [28]. All the methods are described in detail.
4.1. Tinnitus Retraining Therapy (TRT)
Tinnitus retraining therapy is the use of a combination of low level, broadband noise, and counseling for the patient to get habituated to Tinnitus. The overall objective is to divert their mind off Tinnitus. It involves training the nervous system to enhance the sound outside, making Tinnitus noise to be perceived as background noise, which diminishes the jarring effect. It is also known as Acclimatization therapy.
TRT combines medical evaluation, counseling, and sound therapy to successfully treat a majority of patients. Before beginning TRT, there is a preliminary medical evaluation of patients, which is done by taking a questionnaire survey as well as an audiological test [10].
There have been recent developments and research on Tinnitus retraining therapy, which found its roots in neurophysiology and psychology model. Surveys show that using music to regulate and suppress negative emotions is effective. The purpose of music therapy is to inducing relaxation, alleviation of mood, and inculcating a sense of control. Experimental results show that the method has good effects. Music has been able to mask Tinnitus effect according to several patients [4].
According to a research by Carol Bauer et al. [29] 70% of patients treated with Tinnitus retraining therapy (involving hearing aids and counseling) reported moderate to significant improvement in Tinnitus severity while 76% of patients receiving sound generators and counseling endorsed improvement in Tinnitus.
Alejandro Jose Uriz [30] developed a device to mask Tinnitus through filtered noise using a bandpass filter. The system was coupled with a digital assistive listening device that used digital signal processing techniques to obtain the most important features of a high-end commercial assistive device. Not only was the device successful in masking the noise to a fair degree, but the proposed technique also improved the perception of spectrally adjacent sounds to the Tinnitus.
4.1.1. Chaos Theory
Despite the soothing effects of music, there tends to exist an associative memory pattern between Tinnitus noise and music played to mask the sound at a particular instant. There is a huge issue that arises due to this. No matter how soothing or relaxing the music appears to be, it can never reach the expected effect because memory will recall the Tinnitus effect associated with that particular music. Chen Jie-mei et al. [4] proposed a system to solve this issue. They described a system to synthesize music based on chaos for Tinnitus treatment. Music is stated to be a chaotic motion in time series- a gradual transition from order to disorder. It appears to be random, but supposedly, it has an inherent, deep regularity. Chaos is so sensitive to initial conditions that the regional musical works tend to be unstable. Controlling the entire system by chaotic attractor can make the overall musical work tend to be stable. The main idea was to generate notes and rhythm using a chaos algorithm and transmitting this sound through MIDI. Their work concluded that the Tinnitus rehabilitation music, based on chaos proposed in this paper, obeys a regular pattern which appears to be random. The notes that are generated are similar, but never identical to the previous notes. Hence, when the Tinnitus patients undergo this kind of masking therapy, it proves to be more effective and hence, is asserted to be more practical.
4.1.2. Action Rules Extrapolated from Database
Data extracted during clinical TRT sessions, coupled with pre-existing medical records of a patient, may prove to yield meaningful inferences, according to Xin Zhang et al. [10]. They have developed a flexible temporal feature retrieval system connected to an action-rules engine, based on grouping similar patterns of patients visiting TRT centers. An action rule is a rule extracted from a decision system that describes a possible transition of objects from one state to another concerning a distinguished attribute called a decision attribute [31, 32]. They are nothing but a set of protocols followed to facilitate a certain task or set of tasks. A paper published previously [10] describes action rules as authoritative regulations extracted from an information system that describes a possible transition of objects from a particular state to the next, concerning a feature called the decision tree feature. Their system requires a preliminary medical evaluation, after which patient categorization is performed based on the question forms and audiological evaluation, which collects many aspects of the patient’s Tinnitus, sound tolerance, and hearing loss. The evaluation also helps to determine the relative contribution of disorders, such as hyperacusis (increased sensitivity to certain sound frequencies) and misophonia (hatred of sound). A set of questions developed by the authors ask about the activities prevented or affected, such as sleep, work concentration, etc. All responses are included in a database.
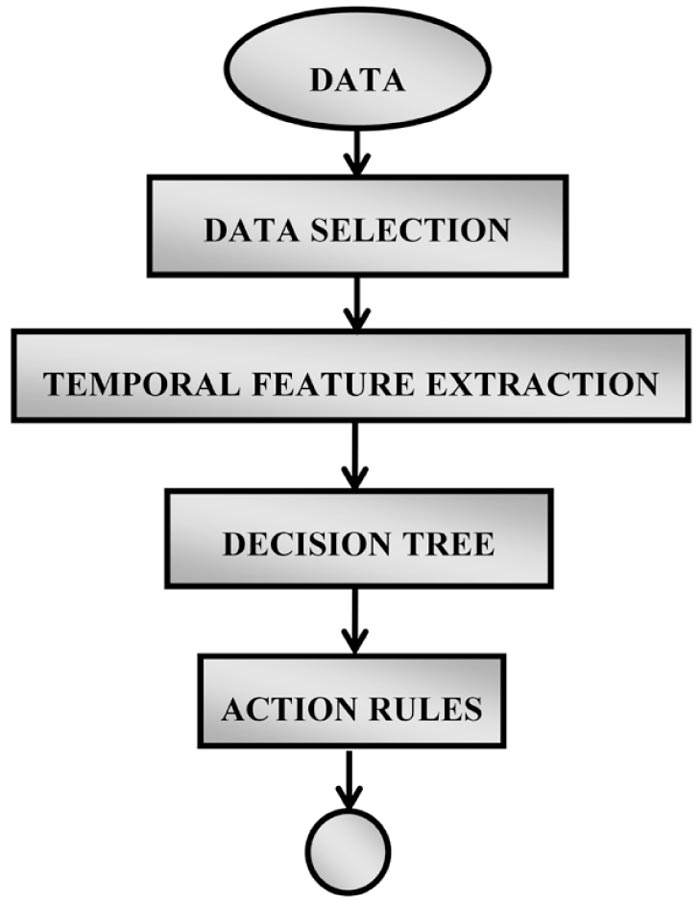
The proposed temporal feature retrieval system was based on grouping the patients of similar visiting frequencies with connection to an action-rules engine. The system consists of four modules, which are shown in Fig. (5).
- A Data grouping device: To filter out less relevant records in terms of visiting duration patterns.
- Temporal feature extraction engine: To project temporal information based, patient-based records for classic classifiers to learn the effects of treatment as well as Tinnitus upon patients
- Decision tree classification device: To generate classification rules
- Action rules generation device: To build action rules from a certain pair of classification rules
The system was successfully modeled with Microsoft access databases as well as WEKA. The authors explored a database of 215 patients, who have at least four visits during the process of the TRT with 32 features. After the research, the authors came up with 6 sets of action rules which are stated as follows:
(1) If patients have hearing loss as a significant subjective problem and Tinnitus as a significant problem, have ‘A1’ of the total score less than 3.7, having real ear measurements in the first visit or not decides if they will have improvements in terms of catastrophe scores after TRT.
(2) If patients have the primary problem of hyperacusis and are treated for this condition with a specific TRT protocol that involves the use of wearable sound generators or combination instruments and have A1 of the total score less than 3.7, the change of follow up method from counseling to telephone indicates improvements in terms of catastrophe scores after TRT. More so, the rule strongly suggests that the telephone method in the mentioned condition means improvements on catastrophe, where the side of the action rule has a support of 13.
(3) If a patient has the primary problem of hyperacusis and is treated for this condition with a specific TRT protocol that involves the use of wearable sound generators or combination instruments and has A1 of the total score less than 1.1, and there is no dependency on the presence of hyperacusis, he or she may have improvements in terms of negative emotions score after TRT.
(4) If a patient has the primary problem of hyperacusis and is treated for this condition with a specific TRT protocol that involves the use of wearable sound generators or combination instruments, and has A1 of the total score less than 1.1 and T2 of the total score less than or equal to 12, the change of the most important problem from hyperacusis to Tinnitus or hearing loss indicates improvement in negative emotions.
(5) If a patient has T1 of the total score not greater than 2 and T2 of the total score not greater than 12, and if Tinnitus is the most important problem in the last visit, stopping the real ear measurements in the second visit means improvement of the negative emotions.
(6) If a patient has T1 of the total score greater than -4 and T2 of the total score not greater than -2 and T2 of the catastrophe greater than -4 and the most important problem of the second visit is either Tinnitus or sound loss, then he or she will have an improvement in terms of functional problems.
In the mentioned rules, A1, T1, and T2 are certain mathematical parameters describing the temporal feature values. The cited paper explains them in detail, along with mathematical assertions of the mentioned rules. We shall omit the mathematics here for the sake of brevity.
4.2. Signal Processing Approaches
Tinnitus has been classified into tonal and noise Tinnitus [28]. For tonal Tinnitus, the frequency is the main characteristic. (50Hz-20000Hz). Noise Tinnitus is harder to characterize. The degrees of freedom, in this case, is the frequency range and also the dynamics in all of the included frequency bands.
Tinnitus signal is different for every patient. The sound that a patient hears may be a single tone (mono-tonal), multi-tonal (many different tones), or have a noisy characteristic [28].
Matthias Lippmann et al. [28] presented new ways for the diagnosis and treatment of mono-tonal and multi-tonal Tinnitus. Due to new music, theoretical approaches, and modern techniques, individual Tinnitus frequency of a patient can be determined accurately. New processing techniques for phase shift treatment of predominant Tinnitus frequencies are presented in the paper. The authors have also developed a handheld device for home therapy along with software for both communications between physician and patient as well as the communication between hand-held devices and clinic systems. They present their research on modeling noise Tinnitus by using pseudo-random sequences. After this modeling, noise cancellation techniques can be used for Tinnitus compensation. The paper states that Tinnitus sound cannot be measured objectively.
Hence, a way of modeling the patient’s individual Tinnitus sound needs to be concocted. For the creation of the model, the therapist and patient must work together for the classification and characterization of Tinnitus sound.
The concept of performing Tinnitus therapy by using the concept incorporated in sound cancellation headphones was already filed for a patent in Dresden Germany, in the year 2002 [33]. Introduced to the medical science community was the procedure in the pioneering paper by Choy in 2004 [34], which used Phase Shift Tinnitus Reduction therapy for treatment purposes.
Since then, a lot of research has been done on this topic to improvise on the results.
The main challenge is to determine the exact timing of the peak and trough of the endogenous wave [28]. In conclusion, the authors to the paper [28] show new ways for diagnosis and therapy of the different kinds of Tinnitus disease.
Algorithms have been developed to improve audiogram measurement and Tinnitus diagnosis. In addition to tonal Tinnitus, using proper filter techniques and pseudo-noise signals, noise Tinnitus can be diagnosed as well [35]. Modern audiogram measurement procedures have a very small resolution in the frequency domain. Diagnosing the Tinnitus frequency or spectrum for noise Tinnitus is necessary for using sound cancellation in Tinnitus therapy. These techniques can now be applied to the patient’s beloved music. They can also be implemented in portable devices. Software applications and hardware prototypes have been developed for both home and clinical treatment and are projected to be available in the market. The next subsection analyzes such portable devices.
4.3. Portable Systems
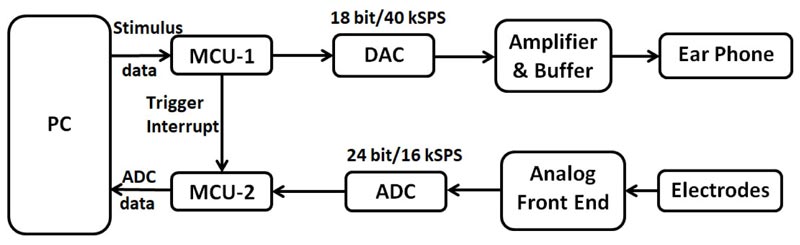
Zheng Linnan et al. [36] depict an Android-based Tinnitus treatment system. They have developed a software, known as TinnitusTreat software, to treat the disorder. It incorporates all the functions in real-time treatment and doctor-patient communication. According to their paper, the primary way of treating Tinnitus is by going to hospitals. However, it is costly and, according to the authors, not conducive for patients to treat themselves anywhere. Thus, the authors have built a practical mobile treatment platform using the android handset (mobile phones). The application performs several functions, such as the acquisition of the Tinnitus therapy sound and personal information from the server. There is also a doctor-patient communication feature and a Tinnitus forum. It is proven to be a stable platform through the results of the paper, and it provides a new idea for Tinnitus portable treatment. In hospitals, masking therapy is most commonly used for Tinnitus treatment because of its unique advantages, such as validity and security. But masking instruments are bulky and expensive, hence the patients must go to the hospitals for treatment. There exist certain internet interrogation softwares, such as the Chun- Yu Doctor and GoodDoctor Online, that facilitate the communication between doctors and patients. The system functionality is described as follows: The first time, when a patient visits the doctor, the doctor will help the patient to match the Tinnitus rehabilitation sound according to the type, frequency, and loudness. After matching the sound, the software at the PC side shall store this data on the database of the server. The android app shall access this data from the server and play the sound for rehabilitation accordingly. The app has other features for communication between the doctor and patient as well. Also, it has a Tinnitus forum module. The app was built successfully. The scalability of the deployment of the system is unknown. The architecture of the system proposed in a previous study [36] is depicted in Fig. (6).

In another piece of work, Muntazir Mehdi et al. [37] developed a mobile app called TinnitusSense that enables therapists and researchers to collect evidence for unknown facts. The app utilizes sensors, which are embedded in common smartphones and attempts at acquiring environmental data and monitors patient activity to understand the correlation between Tinnitus symptoms with changes in the weather. Currently, it relies on user-entered data for measuring the impact of the user’s Tinnitus. It proposes the addition of mobile EEG systems coupled with smartphones to acquire electrical activity of the brain and enable real-time neurofeedback to the patients suffering from Tinnitus.
The future may attract several such IoT based systems for Tinnitus research.
4.4. Neuromodulation and Stimulation
Acoustic Coordinated Reset (CR) neuromodulation is a technique that minimizes the hyperactivity in the specific areas of the brain, which are responsible for the generation of Tinnitus sound. It involves complex mathematical algorithms that produce sounds pertinent to a unique individual. These produced audio signals disrupt the synchrony in the region, resulting in Tinnitus. Efforts are being made to not affect normal hearing during this kind of therapy.
In Acoustic CR Neuro-modulation, the synchronous nerve cell network is first simulated from outside by single tones that are specially targeted, this forces the cells into subgroups, each with its new rhythm. Four tones are used to deliver this gentle targeted stimulation to the hearing center of the brain. There are short pauses between the stimulation signals to remodel the network. If repeated, these stimulation signals will reduce the hyperactivity to such an extent that the abnormal neural synchrony will be permanently reversed.
Acoustic CR neuro-modulation tones consist of individually measured and specifically calculated acoustic impulses, which transformed in the brain in corresponding electrical stimuli. The acoustic tones are generated by a small device and administrated to the patient by a headphone worn for 4-6 hours a day.
The signals are targeted by taking advantage of the keyboard like the structure of the auditory center. The area generating the Tinnitus is found by determining each pitch of Tinnitus of the patient. Now, the Acoustic CR neuro-modulations can be guided selectively to the right place. Here, it produces a reversal in the neural synchrony [38].
A survey conducted by Tinnitus Centre Munich, Germany, shows that despite the small number of patients (about 25) and shorter duration of the study (4 months) Acoustic CR neuromodulation has a remarkable response rate of 72%.
The main issue with this treatment is its extremely high cost. On average, it may cost over 5000 US dollars [39], which is unaffordable for the majority of the population. Also, the method takes time for patients to adapt to. It is not universal and is patient specific.
Furthermore, according to a detailed Literature survey on Acoustic CR neuromodulation, it was concluded that although the limited level of evidence suggests that acoustic CR neuromodulation may have positive effects on Tinnitus symptoms, the available evidence is not sufficient for the scalable clinical implementation of this method [40].
Another piece of related work was “Neuromodulation of the Striatum for Treatment of Refractory Tinnitus” conducted by Paul Larson et al. [41], aimed at controlling the unwanted sounds generated in the central auditory system and prevent them from reaching conscious awareness.
Transient simulation of the striatum was performed during routine Deep Brain Stimulation (DBS) implantation on various subjects. In 5 of the 6 subjects with Tinnitus where the DBS lead traversed the striatum, Tinnitus loudness was suppressed to level 2 or lower on a 0 to 10 rating scale. In the sixth subject who did not have a reduction in Tinnitus, the lead was outside the striatum. Induction of new phantom auditory percepts or modulation of baseline Tinnitus sound quality during stimulation was observed in 3 patients with and 2 patients without comorbid Tinnitus. No subjects had new hearing loss during or after striatal stimulation.
They concluded that phantom auditory disorders, such as Tinnitus, may be viewed as pathologic permissiveness of striatal gating function. Neuromodulation of the striatum appeared to be interrupting the perceptual integration of phantom sensations generated in the central auditory system. This new, non-auditory-based treatment approach deviates from the more prominent audition-based solutions.
Hamidreza Abtahi et al. [42] conducted a study on Transcranial Direct Current Stimulation effects on Tinnitus. They performed anodal, cathodal, and control stimulation to the brains of a group of 51 patients with Tinnitus – sustaining 20-min current stimulation of 2mA. The subjects received weekly transcranial electrical stimulation for two months, and their long-term recovery from Tinnitus was investigated. They concluded that anodal stimulation effectively reduced Tinnitus in the short term, in contrast to cathodal and control stimulations, which had milder effects.
While many pieces of research pertinent to neuromodulation and brain stimulation have yielded positive results, there have been numerous failed attempts in this domain, which were unable to provide any conclusive solution. For example, Julien Engelhardt et al. [43] performed research to evaluate the efficacy of chronic electrical epidural stimulation of the auditory cortex on severe and disabling Tinnitus. Their study, however, did not find an objective efficiency of chronic cortical stimulation for severe and resistant Tinnitus.
4.5. Miscellaneous Work
Without the knowledge of Tinnitus signal patterns and study of the signals responsible for the Tinnitus noise itself, it is very difficult to find effective treatment methods. This sub-section documents the study of the signals associated with Tinnitus noise and system modeling to suppress it, along with other surveys and summarization.
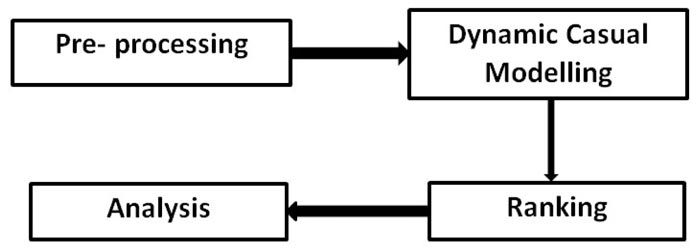
There may be future scope for research in Tinnitus detection and treatment by reading and manipulation of EEG signals from the auditory cortex. There has been a vast amount of research done in correlating Tinnitus Noise with EEG signals [44, 45]. A good amount of research has been done on localizing the area of the brain, which is responsible for Tinnitus. An algorithm based on Dynamic Causal Modeling (DCM) and Exponential Ranking [46] has been tried and tested. The system flow for DCM is shown in Fig. (7).
Yunseo Ku et al. [47] documented their work done in the development of a PC based single platform for objective Tinnitus diagnosis research to record AEP(Auditory Evoked potential), which was synchronized to the specific acoustic stimuli of the GPI method. The system that they developed was feasible for the further study that finds optimal parameters of the acoustic stimuli and the diagnosis features in various AEP waves. “Tinnitus is the subjective perception of sound with no physical acoustic stimulus in the ears.” Tinnitus diagnosis and treatment currently relies on “self-reporting”. For the assessment of objective Tinnitus, “Gap prepulse inhibition of acoustic startle” (GPIAS) method was proposed and has been evaluated in some animal studies. The AEP based system model is given in Fig. (6).
EEG has become a standard brain-imaging tool to quantify and even qualify neural activities of the brain, which are mainly spatial, spectral, and temporal patterns associated with the different processes like motor, emotional and cognitive. Tinnitus patients with high extreme distress display an increase in the activity of the EEG in the oscillatory range, i.e., around 25Hz, which corresponds to the upper beta band of the EEG signal over the frontal recording sites. Whereas moderate to high presence of Tinnitus in patients show an enhancement in EEG signal activity within the range of delta, alpha, and lower gamma bandwidths [48]. The auditory system is responsible for hearing and balance. Therefore, such disturbances in the EEG patterns caused due to Tinnitus not only affect the mental peace but also result in balance disorders.
Maroof H. Choudhury and Armando Barreto [49] proposed a recording system for the study of Tinnitus through Auditory Evoked Potentials. The investigation of EEG related to Tinnitus requires analysis of AEP signals, including long latency features. Regular AEP measurement instruments for audiometric screening are limited in their capabilities to record these features. Thus, the authors have developed an AEP measurement system featuring extensive flexibility and configurability to study the EEG correlates of Tinnitus. The work concludes that the pitch of Tinnitus in noise-induced hearing loss frequently correlates with the characteristic frequency of the firing rate of neurons innervating the inner hair cells of noise-damaged regions. Different types of destructive surgery, including neurectomy, failed to improve or abolish Tinnitus (Fig. 8).
| S. No. | List of Questions used to interview Audiologists and Neurologists |
|---|---|
| 1 | Name |
| 2 | Date |
| 3 | Profession |
| 4 | Hospital |
| 5 | How many Chronic Tinnitus cases do you see in a month? |
| 6 | What proportion of these cases has predominant frequency/single frequency Tinnitus? |
| 7 | What, according to you, is the most effective management for chronic Tinnitus? |
| 8 | Do you think that noise cancellation by phase-shifting will alleviate the continuous ringing sensation? |
| 9 | Reasons if you think that the noise cancellation will work |
| 10 | Reasons if you think that noise cancellation will not work |
| 11 | Reasons for lack of confidence in the above stance |
| 12 | Recommendation on how to carry out a study to test the noise cancellation system on patients |
| 13 | Any other feedback or comments |
| Method | Advantages | Disadvantages |
|---|---|---|
| Tinnitus retraining therapy(TRT) and white noise masking [10] | Provides alleviation from Tinnitus to some extent by causing the patient to stop focusing on the Tinnitus noise | Affects normal hearing, risk of the human brain to recall Tinnitus associated with sound, Inaccurate results |
| Synthesizing music for Tinnitus treatment based on the chaos [4] |
No issue of patient recalling Tinnitus sound associated with a particular kind of music | Affects normal hearing |
| Android Based Treatment Method [23] |
Portable, easy communication and monitoring between doctor and patient | Lack of accuracy in suppression |
| Signal Processing and System Design for Tinnitus Treatment [28] |
Better accuracy in Tinnitus suppression |
Lacks accuracy in comparison to recent, advanced methods, Lacks scalability Model |
| Acoustic CR Neuromodulation [38] |
One of the most accurate Tinnitus suppression methods currently in existence | Extremely and unfeasibly high cost |
| Medication [8] | Does not require bulky equipment to be attached to the body at all times | Causes severe side effects and reduces the effect only to a certain extent. Also, medication does not work in all cases |
5. DISCUSSION
At present, we have technologies or drugs that can only reduce the effect of Tinnitus but not completely cure it. Furthermore, these techniques are accompanied by several drawbacks. They continue to affect normal hearing, do not remove Tinnitus noise to a considerable extent, or are absurdly expensive. The amount of people suffering from it is constantly growing. The number of suicide cases due to severe Tinnitus is also on the rise. A solution that can completely cure the issue of Tinnitus or at least reduce it to such an extent where a person can work without any stress or pain is the need of the hour. Moreover, a solution that does not affect the day to day activities, including normal hearing, is required. Most of all, there is a requirement for an affordable solution, which can make the treatment accessible to one and all.
Apart from work done in the technical field to overcome Tinnitus symptoms, a few surveys have been carried out as well, to hear from doctors and clinical specialists about their understanding of Tinnitus. It is highly essential to have intact communication between clinical specialists and biomedical developers for there to be sustained progress in research. Darien Rodriguez et al., in their paper [50], have presented statistics and survey data on their work done in Predominant Tonal Tinnitus (PTT) suppression using a sequential phase shift approach. PTT is a particular type of Tinnitus involving the occurrence of a single persistent frequency with varying phase and magnitude. They make use of a Tinnitus noise-generating tool, which tries to identify the specific Tinnitus frequency through several tests. Again, this identification is done by verbal confirmation of the patient as to whether or not the produced sound is similar to the Tinnitus of the patient. Table 2 shows the questionnaire proposed in a previous study [50].
Imminent work of research may choose to adopt a similar questionnaire model for communication and survey purposes. These survey questions were used to validate the process of testing the software solution for patients. Depending on the feedback, the audiologists were able to categorize the type of Tinnitus.
Mayo Clinic [8] has summarized the various treatment methods of Tinnitus by classifying them into three categories:
- Treating an underlying health condition: Many times, an underlying medical condition is associated with the cause of Tinnitus symptoms. The doctor shall first consider diagnosing this condition, and if found to yield positive results, shall attempt to treat it by taking steps such as removal of earwax, treatment of a blood vessel condition(requiring surgery or other methods to address the problem), changing the medication that may appear to be the cause of Tinnitus, etc.
- Noise suppression: Includes usage of white noise machines and masking devices – which produce simulated environmental sounds, hearing aids – to amplify actual external sound in contrast to Tinnitus noise, and Tinnitus Retraining Therapy (TRT), which produces tonal music to mask the specific frequencies of Tinnitus and make the patient accustomed to the sound.
- Medications: To reduce the severity of symptoms and complications, possible medication may include Tricyclic anti-depressants. They have yielded decent results. However, they cause troublesome side effects, including constipation and heart problems, hence are generally used only if Tinnitus is severe and unbearable. Xanax medication can also be used, but they come with side effects such as drowsiness and nausea as well. They may also turn into habit forming drugs. These drugs can only help reduce the severity of symptoms in some cases, and cannot cure Tinnitus.
The following Table 3 highlights the primary advantages of the various pieces of work mentioned in this section.
CONCLUSION
This review article summarizes the causes and impacts of Tinnitus. This is significant because it addresses and creates awareness for people about the various mental and physical health problems related to Tinnitus and why one should take pro-active measures to deal with it. At the same time, it also elaborates the existing solutions and highlights their various pros and cons.
Despite, extensive amounts of research work, there is no robust solution to overcome Tinnitus. It looks like Tinnitus will continue to be a part of the present world and, without a doubt, will continue to attract substantial clinical and research contributions from clinicians and technologists, as no cure has still been found to completely eradicate the cause. At present, technologies or drugs are available, which can only reduce the effect of Tinnitus but not completely cure it. The amount of people suffering from it has constantly been growing. The number of suicide cases due to Tinnitus is also on the rise.
Through the first half of this article, an attempt was made to spread awareness about the disorder. Tinnitus should not be confused with schizophrenia or other phantom auditory disorders. Neither should it be neglected. Through a detailed summarization of the advances in treatment methods in the latter half of the paper, readers are provided with a catalog that may bolster further innovations.
This review article would interest people suffering from Tinnitus and also to the scientist or doctors working in the field of Tinnitus.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
This review was carried out with the funding assistance received as Student Startup Venture Initiative 2018-19, coordinated by VIT-Technology Business Incubator (VITTBI), supported by VIT Vellore and the grant release is through the Entrepreneurship Cell, VIT.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

